Have you been told that your thyroid tests are normal, but you still wonder if something is not right?
Are you confused with all of the test names and result ranges?
Let me help you understand what those tests mean, and what they mean for you.
The brain controls how much thyroid hormone is produced by the thyroid gland. The hypothalamus produces Thyroid Releasing Hormone (TRH) to tell the pituitary to make another signaling hormone, Thyroid Stimulating Hormone (TSH). We don’t test TRH levels in the average patient because we get the information we need from other thyroid tests.
TSH then stimulates the thyroid gland to make thyroid hormone. When the brain decides that the body needs more thyroid hormone, TSH levels go up. If there is too much thyroid hormone, TSH levels go down.
The thyroid makes several thyroid hormones, designated T1, T2, T3, and T4 because of the number of iodine ions on each thyroid hormone molecule. We generally only pay attention to T3 and T4; we are not really sure what functions T1 and T2 have so we don’t measure them in the clinical setting.
T3 is the more active hormone, but it is harder to measure. T4 is the less active hormone, but it is easier to measure.
The thyroid gland makes primarily the inactive T4. Those T4 molecules then travel to the liver, the GI tract, and the rest of the body to be converted into T3.
Thyroid hormones occur in two forms: free or bound. Hormones in general travel around the body attached to various binding proteins, but in their bound state are not ready to work (inactive). The active hormone is the free hormone. You can measure free T4 and free T3, you can also measure total T4 or total T3, which is the sum of both the free and bound components.
There is also reverse T3, which is an inactive form of T3. Normally, we all make a small amount of reverse T3, but if you are sick, stressed or inflamed, you may make more. This is the body’s way of conserving energy in times of illness. Many people have chronic health problems (diabetes, hypertension, asthma, etc.), and even these kinds of chronic diseases may stimulate your body to make more reverse T3. In that case, even if your TSH is normal, you may not have enough of the active, or free, T3 to keep you feeling energetic. I find that many of my patients feel better when taking a combination of T4 and T3, or even just T3 alone, especially if reverse T3 is very high.
In the US today, the most common cause of hypothyroidism (underactive thyroid) is an autoimmune problem called Hashimoto’s thyroiditis. You can measure antibodies to the thyroid gland in a simple blood test. The most commonly measured antithyroid antibodies are antithyroperoxidase (antiTPO) and antithyroglobulin (antiTG). If either of the levels are elevated, that confirms that you have Hashimoto’s. If thyroid antibodies are normal, unfortunately it’s harder to be sure that you don’t have Hashimoto’s. There are a number of other antibodies to the thyroid gland that we know of, but these tests are not available for the average patient; they are used in research settings only. For a person suspected of Graves’ disease, measuring the Thyroid Stimulating Immunogloblulin (TSI) is useful, and will confirm Graves’ if elevated.
If your antibodies are negative, you can request a thyroid ultrasound. The thyroid gland of a patient with Hashimoto’s has a very typical appearance, and can help confirm a diagnosis. A biopsy will help, but I don’t recommend a biopsy for just diagnosing Hashimoto’s.
Lab ranges for normal differ slightly between labs, but the reference ranges are always printed on the lab slip next to your test result.
What you must know is that most lab reference ranges are out of date with the science. About 15 years ago, researchers looked at the reference population for this test, and when they eliminated everyone known to have autoimmune thyroid disease from the “normal” group, they found that most normal people had TSH levels between 0.5-2.5. Many labs still use reference ranges up to 4.8 or 5.5, which I believe is abnormal. Most functional medicine practitioners (including me) believe that an optimal TSH is between 1-2.
Ultimately, an astute clinician will always interpret test results in light of the patient’s problems. Some people may feel better with levels at the higher or lower end of normal.
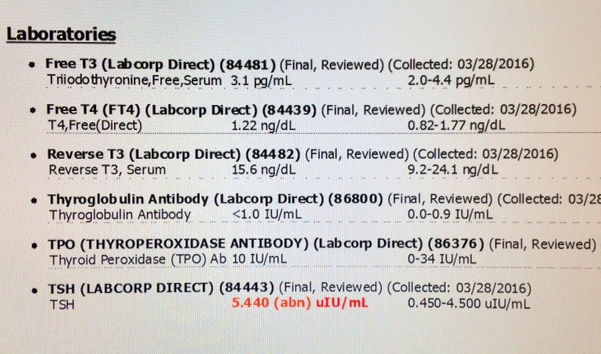
Many doctors will only order a Thyroid Stimulating Hormone (TSH) to assess thyroid function. I believe that a full assessment of the thyroid gland should include the following tests:
- Free T4
- Free T3
- Reverse T3
- TSH
- Antithyroid antibodies (antiTPO and antiTG)
- Ferritin (this is a measure of iron storage; iron is necessary for normal thyroid hormone production)
If you are taking thyroid hormone, the timing of your blood test is important. Thyroid hormone levels fluctuate during the day, so ideally, get your blood drawn 6-10 hours after taking your last dose of thyroid hormone (midafternoon for most people).
To your health,
Patty Powers, MD
Facebook: Patty Powers MD